Pulmonary arterial hypertension
My dear father, had scleroderma with pulmonary hypertension. He told me that he had a small atrial problem and was guven option whether should do or closure or not?
This was in 2002, around there. 2 years after spm. Had done his right heart cath told me that his right heart pressure was high. He told me that his lungs were fibrosed and thus causing it to have back pressure to the right heart chambers.
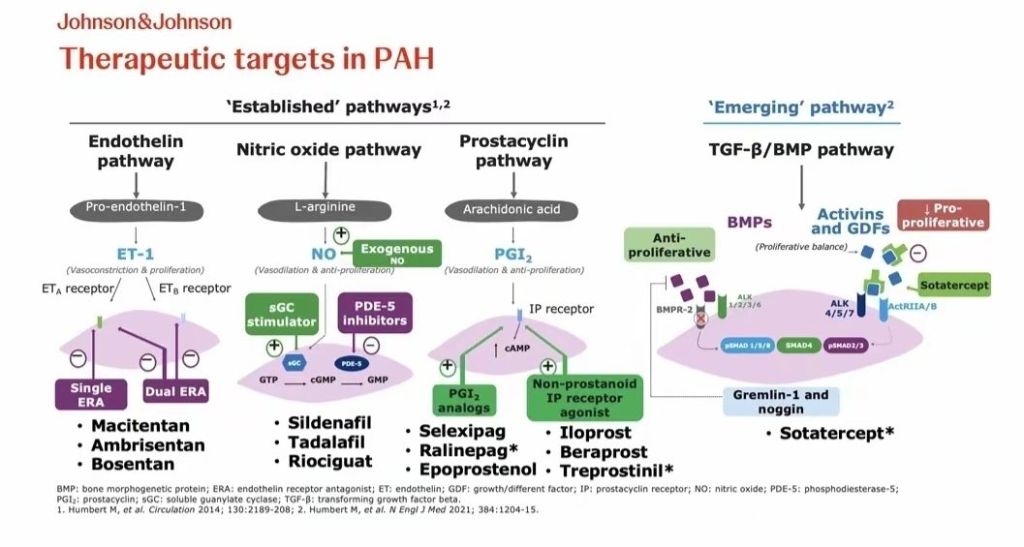
Had talked with him in regards to bosentan, sildenafil and ilioprost. Herm.
He showed me the echo finding. Didnt know much at the time because no one knew and no one understands. Heck i didnt know who or what to ask also.
Followed him with his appointment. was with him in the echo room. Even then when he wanted to do cardiac mri, a doctor called me from the hospital that his heart rate was elevated and couldnt proceed.
He told me he has one of a kind problem. He had asd. But knowing this, i merely thought asd as congenital heart disease, but he had a special kind, an acquired asd.
..
He had everything, ogds, renal biopsy, right cath study, echo this and that, lu g function this and that, macam macam blood test. Cardio, resp, rheumato, radio.
..
Acquired ASD in Scleroderma-associated Pulmonary Hypertension
Acquired Right-to-Left Interatrial Shunting in Systemic Sclerosis with Severe Pulmonary Arterial Hypertension
Systemic sclerosis is a multisystem autoimmune disease associated with vascular dysfunction and fibrosis. One major cardiopulmonary complication is Pulmonary arterial hypertension. Severe elevation of right-sided pressures may unmask or enlarge a previously silent interatrial communication, producing an acquired ASD physiology.
Case Presentation
A 50 somethinyear-old man with known diffuse systemic sclerosis for years presented with progressive exertional dyspnea, lower limb swelling, and reduced exercise tolerance over months.
occasional chest discomfort,
Markrd exertional dizziness,
worsening fatigue,
Raynaud phenomenon,
interstitial lung disease,
gastroesophageal reflux disease.
On examination:
BP 120/68 mmHg,
pulse 102 bpm,
oxygen saturation 89% on room air, 6mwt result pun tak ingat lah
JVP tak elevated pun dulu.
loud P2,
bilateral pedal edema.
Investigations
Bloods
BNP elevated
ANA positive
Anti-centromere antibody positive
Anti topoisomerase postive anti scl
ECG
Right axis deviation
RV hypertrophy
Chest X-ray tak ingat
Cardiomegaly
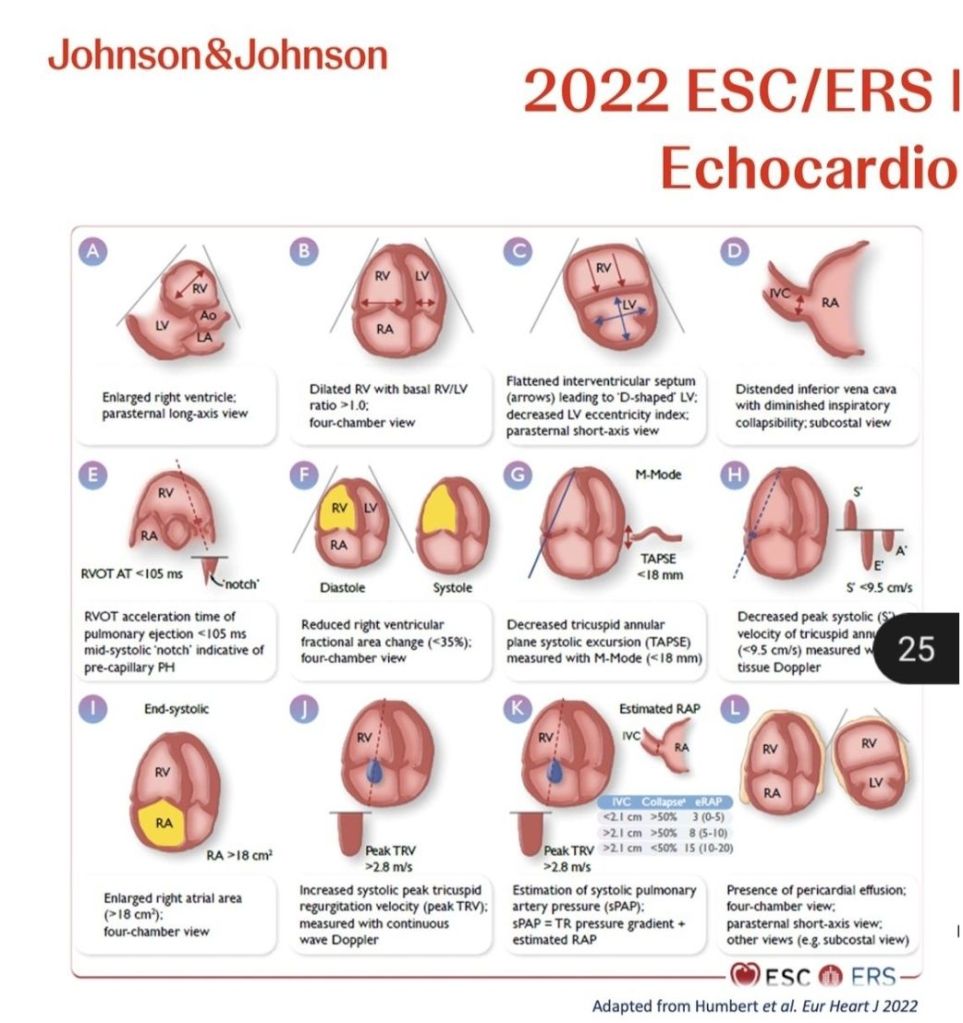
Echocardiography
Findings showed:
severely dilated right atrium and right ventricle,
severe tricuspid regurgitation,
estimated pulmonary artery systolic pressure of 80 mmHg, rvsp 75
small interatrial septal defect
Right Heart Catheterization
Confirmed severe pulmonary arterial hypertension:
mean PAP: 48 mmHg,
elevated PVR,
normal wedge pressure.
Discussion
In systemic sclerosis, pulmonary vascular remodeling may progressively increase right-sided cardiac pressures. This can lead to reopening of a previously silent patent foramen ovale or enlargement of a small atrial septal communication, producing clinically significant shunting.
The patient’s hypoxemia and worsening exercise tolerance were likely secondary to:
severe PAH, right ventricular failure,
right-to-left interatrial shunting.
Closure of the ASD was not immediately pursued due to concern that the shunt functioned as a “pop-off” mechanism for severe right-sided pressures.
Management
The patient was started on:
diuretics, oxygen therapy, we got 3 machine LTOT. Kat kampung, bilik dan dah rosak. sildenafil, dulu pfizer original, sekarang ada generic ..endothelin receptor antagonist therapy. I know there is a new one now.
pulmonary hypertension specialist center for advanced therapy evaluation.
Conclusion
This case highlights the importance of considering interatrial shunting in patients with systemic sclerosis and severe pulmonary hypertension presenting with worsening hypoxemia. Apparent “acquired ASD” physiology may arise from pressure-mediated reopening of latent interatrial communications.
…
I leared that patient will have adapted physiology. Not your normal physiology but adapted physiology. Different readings, different normal values, different adapted physiology.
Kalau bahasa moden macam neuroplasticity lah.
Tapi homeostatsis can be variable.
Hahah..
…
My thoughts. Wrote here because it has been quite a while in my head.
Just want to say thank you Abah.
Thank you.




Leave a comment