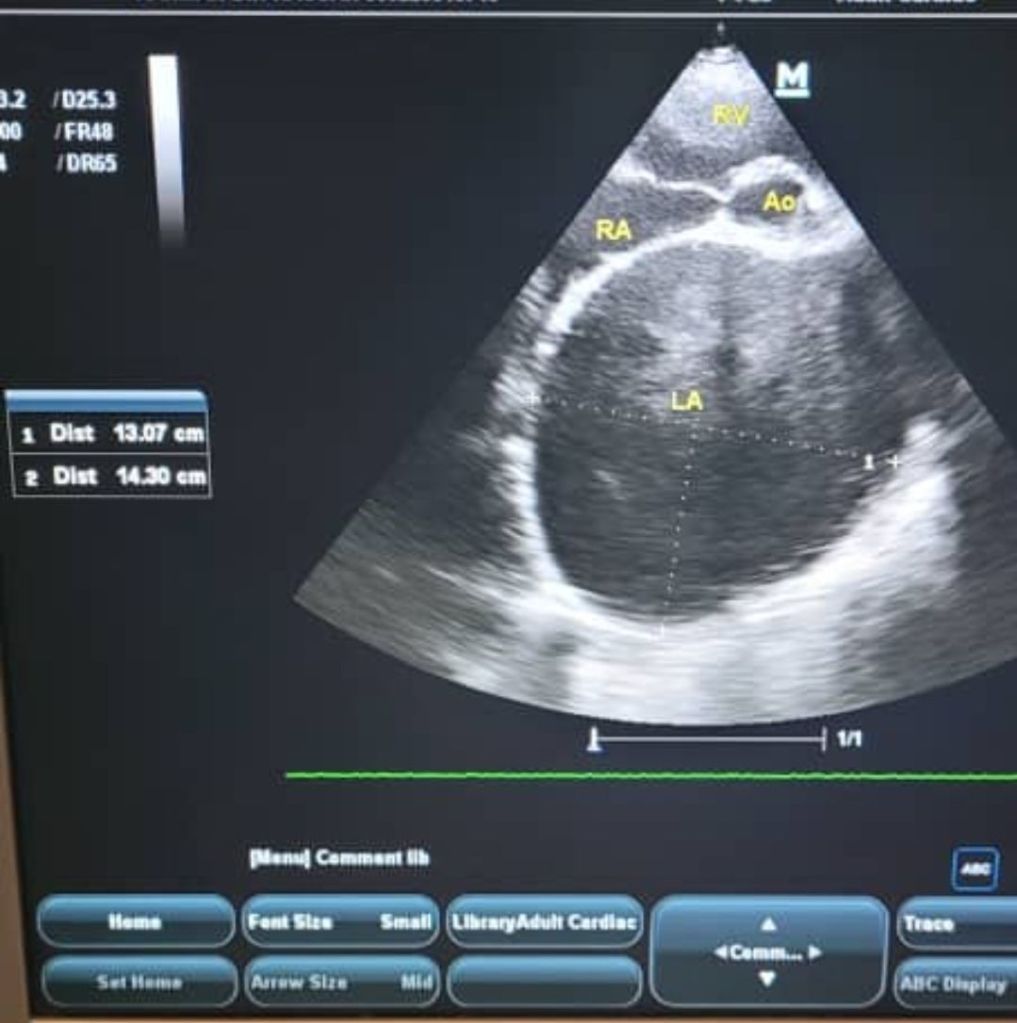
Super dilated LA
Learning for today. Did not publish this case because exam that time. Keep it here for my personal reading.
Simulated learning with Deepseek.
Unpublished.
..
Progressive Dyspnea in a Patient with Prior Mitral Valve Replacement
Patient: 64 year-old male
History:
· Rheumatic heart disease since childhood
· 15 years ago: Underwent mitral valve replacement (MVR) for severe mitral stenosis. Metallic i guess.
· 5 years ago: Developed permanent atrial fibrillation was on Warfarin. Did not take for 2 years. 2 years off.
· 3 months ago: Gradual onset of dyspnea on exertion (now NYHA class III)
Presenting symptoms:
· Orthopnea, paroxysmal nocturnal dyspnea
Examination:
· BP 130/70, HR 88 (irregularly irregular)
· JVP elevated (12 cm H₂O)
· Auscultation: Muffled prosthetic valve sounds; soft systolic murmur at apex
· Bilateral basal crackles, mild pedal edema
Investigations:
· Echocardiogram:
· Left atrial volume index: 90 mL/m² (severe dilation, normal < 34)
· Mitral valve mean gradient: 14 mmHg (severe stenosis, normal 3–6 for bioprosthesis)
· Valve area (PHT method): 0.9 cm²
· PASP: 65 mmHg (severe pulmonary hypertension)
· LVEF: 55% (preserved)
· LA appendage: Spontaneous echo contrast (no thrombus)
… dunno about this.
· Fluoroscopy: Reduced leaflet motion (structural valve degeneration, not thrombosis)
· CT: No pannus; left atrium 14 cm in diameter
Diagnosis:
Super dilated left atrium secondary to structural valve deterioration of a bioprosthetic mitral valve, causing severe prosthetic stenosis.
Outcome:
Lost to follow up.
According to Deepseek.
(The patient was referred for valve-in-valve (ViV) transcatheter mitral valve replacement given high surgical risk (STS score 9%)
Need to read up on this
Coz i dunno.
. Post-procedure, mean gradient fell to 5 mmHg, and symptoms improved to NYHA class II. The LA remained dilated, but no further enlargement occurred.)
Key takeaway:
A super dilated LA (volume index > 60 mL/m² or diameter > 7 cm) often indicates long-standing, high-pressure LA overload. In this case, prosthetic mitral stenosis caused chronic LA pressure elevation, driving massive dilation despite prior surgery.
Causes of LA dilatation.
Based on your previous question about a super dilated left atrium (LA), you are likely asking why a mitral valve replacement (MVR) can “fail” due to stenosis, and how that leads to the LA becoming massively enlarged again.
Even after successful surgery, the replacement valve itself can develop problems. Here is the breakdown:
Mechanisms of Prosthetic Valve Stenosis
Prosthetic valves can narrow (stenose) due to several factors. The cause often depends on the type of valve implanted:
· Bioprosthetic (Tissue) Valves: These primarily fail due to Structural Valve Deterioration (SVD). Over 10-15 years, the tissue can calcify, thicken, or tear, leading to stiffness and obstruction .
· Mechanical Valves: These rarely degenerate but can obstruct due to Pannus Formation (excessive scar tissue growth) or Thrombosis (blood clot formation) .
· Both Types: Patient-Prosthesis Mismatch can occur if the replacement valve is too small for the patient’s body size, creating a residual gradient .
How Stenosis Leads to “Super Dilation”
If a replacement valve becomes stenotic, the heart is forced to deal with the same problem as before surgery:
1. Blocked Flow: The narrowed valve obstructs blood flow from the LA to the left ventricle (LV).
2. Pressure Build-Up: The LA must generate dangerously high pressure to push blood through the tight valve.
3. Chamber Enlargement: To survive the high pressure, the LA dilates massively. This can lead to failure even if the “new” valve looks structurally intact on an echo .
Clinical Reality: This is seen in long-term cases. For example, a patient with rheumatic disease may have MVR but still develop a Giant Left Atrium (160mm or larger) years later because AF or subclinical valve issues persist .
⚠️ Clinical Signs & Diagnosis
· Symptoms: Return of shortness of breath, fatigue, or palpitations (similar to pre-surgery symptoms).
· Key Tests: Transthoracic Echocardiography (TTE) is the first step. Fluoroscopy helps assess mechanical leaflet movement, and Transesophageal Echo (TEE)/CT is used to differentiate pannus from thrombus .
️ Management Options
Management depends on the cause and surgical risk:
· Thrombosis: Treated with anticoagulation or thrombolytics.
· Structural Failure/Pannus: May require Redo Valve Replacement or transcatheter Valve-in-Valve (ViV) therapy .
· Severe LA Enlargement: If the atrium is compressing the lungs (causing collapse) or the heart, surgical LA reduction (volume reduction procedure) may be performed alongside redo surgery .
In summary: Stenosis of a replacement valve throws the heart back into a state of high pressure, driving the left atrium to dilate into the “super” or “giant” category, often requiring re-intervention.
LA hypertension.
This patient was real.



Leave a comment